
TL;DR
Snow blindness, or photokeratitis, is a painful UV burn of the cornea often caused by sun reflecting off snow, ice, or sand. Symptoms include intense eye pain, tearing, and light sensitivity but usually resolve in 1–3 days with supportive care. Prevention relies on high-quality UV-blocking eyewear and sun safety.
Executive Summary
Snow blindness – or photokeratitis – is essentially a sunburn of the cornea, caused by acute overexposure to ultraviolet (UV) radiation. It occurs when UV rays (primarily UV-B wavelengths) are absorbed by the corneal epithelium, inducing cell death and sloughing of the surface layer[1][2]. This exposes sensitive subepithelial nerves, producing intense bilateral eye pain, foreign-body sensation, and light sensitivity[3][4]. Symptoms typically begin hours (commonly 4–12 hours) after exposure and peak within the first day; the condition resolves within 1–3 days as the cornea heals[5][6].
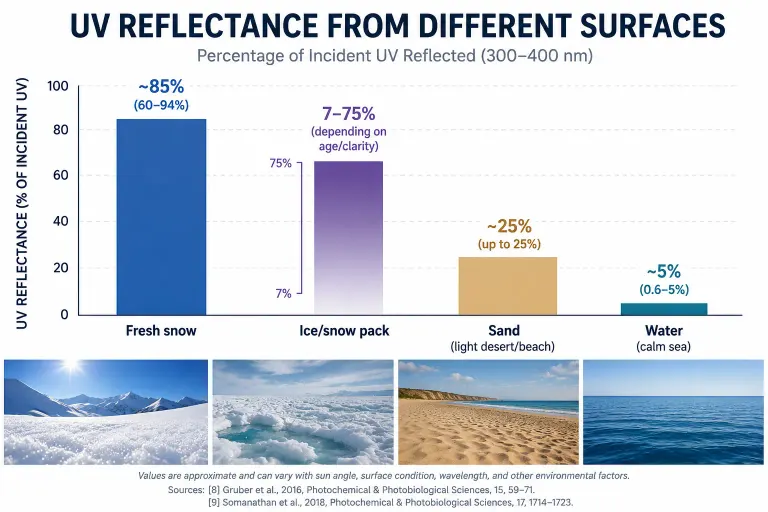
Risk factors are well characterized: high-altitude sun, bright reflective terrain, and lack of eye protection. At altitude, UV intensity rises ~9–24% per 1000 m (strongest for shorter UV wavelengths)[7]. Fresh snow can reflect 60–90% of incoming UV, ice and sand also reflect substantially, whereas water reflects only a few percent[8][9]. Even on cloudy days, scattered UV can reach the eyes. Typical victims are skiers, mountaineers, skaters or beachgoers without UV-blocking eyewear[10][11]. Chronic UV exposure (from many such episodes) raises long-term risks (cataract, pterygium, eyelid cancers) even though an isolated photokeratitis event usually leaves no permanent damage[12][13].
Patients experience excruciating, gritty eye pain (“like sand” or “soap in my eyes”) plus extreme photophobia and tearing[4][3]. Many report inability to keep their eyes open, severe headaches, and anxiety during the acute phase[14][15]. Objective exam reveals red injected eyes and, under a slit lamp with fluorescein, punctate epithelial erosions scattered across the cornea[16][17]. Treatment is supportive: dark room, cool compresses, lubricating drops or ointments and oral pain relief[6][18]. Antibiotic ointment is used prophylactically; eye patching and topical anesthetics are avoided. With appropriate care, symptoms vanish as the epithelium regenerates (usually within 24–72 hours)[6][19]. Prevention is key: high-quality UV-blocking glasses or goggles (UV400 rating, wrap-around style) and other sun precautions dramatically reduce risk[20][21].
Definition and Pathophysiology
Photokeratitis (UV keratitis) is acute corneal inflammation from UV overexposure[22]. It can come from the sun or artificial UV sources (welding arcs, UV lamps). By definition the corneal epithelium – the outermost 50-micron layer – absorbs the bulk of UV (especially 280–320 nm UV-B) and is severely injured[16][23]. At the time of exposure, corneal sensation is paradoxically transiently reduced[24], but damaged epithelial cells begin to die over the next 2–3 hours. As the surface cells slough off, exposed nerve endings trigger intense pain[1][25]. (By contrast, UV-C is normally blocked by ozone, and ~95% of UV-B is also filtered in the atmosphere[26], but strong sun at altitude or reflections can overcome this.) In sum, photokeratitis is literally a “sunburn of the eye”[3]: UV energy causes corneal cell death and inflammation, leaving a raw, abraded surface. Patients often describe it as feeling like sand or grit under the lids[4].
Biologically, UV-B energy (~300 nm) is especially potent. For example, a 300 nm photon has roughly 600× the corneal damaging power of a 325 nm photon[27]. Thus, even though UV-B constitutes a small fraction of sunlight at ground level, its high energy drives the damage. (UV-A, which makes up ~95% of ground-level UV[26], penetrates deeper but is largely absorbed by cornea and lens; it can contribute if intense.) In severe exposures (e.g. welding flash), damage can extend into stromal cells as well. Notably, after initial exposure the cornea’s photoreceptors “reset”, explaining the delayed onset of pain[24].
Risk Factors and Environmental Triggers
Key risk factors amplify UV exposure to the eyes. These include:
- High altitude. UV intensity rises sharply with elevation (roughly +9–24% per 1000 m, more so for shorter UV wavelengths)[7]. Mountain climbers and pilots are at especially high risk.
- Reflective surfaces. Snow and ice act like mirrors for UV. Fresh snow can reflect on the order of 60–90% of UV rays[8], and even aged snow or glacier ice still reflect a large fraction. Bright sand (beaches, dunes) can reflect ~25%[8]. Water at normal angles reflects only a few percent (≈0.6–5%[9]), but at very shallow angles water can still produce glare. In practice, being on snow or near water/sand can nearly double UV eye-dose.
- Time of day/solar angle. UV is strongest around midday and also has morning/afternoon peaks when the sun is low and surfaces reflect upward into the eyes[28]. Solar elevation, clear skies, and lower latitudes (toward equator) all increase UV exposure. Clouds block visible light but not UV very well, so overcast conditions can still produce photokeratitis, especially off bright surfaces.
- Lack of eye protection. Failing to wear adequate goggles or sunglasses in high-UV settings is an obvious risk. Regular eyeglasses without UV coating offer minimal protection. (Welders require special filters, and failure to use them results in “welder’s flash” – essentially identical photokeratitis.)
- Photosensitizing medications. Certain drugs (e.g. tetracycline antibiotics, sulfonamides, some diuretics and acne medications) can increase ocular light sensitivity. While not a primary cause, such medications can lower the UV dose threshold for injury, especially if unprotected in strong sunlight or near reflective surfaces[29].
Cloud cover, atmospheric clarity, and even environment (snowfields in valleys vs. open plains) modulate dose. For example, alpine air (low aerosol/ozone column) increases short-wavelength UV penetration[7]. Any behavior that extends outdoor UV exposure – e.g. skiing all day on sunny slopes without breaks – compounds risk. Protective behaviors (sunglasses, hats) significantly reduce risk[20][21]. Notably, ancestral Inuit communities historically managed this risk with narrow-slit snow goggles (carved antler) to sharply limit incoming light[30].
Symptom Onset and Clinical Course
Photokeratitis has a characteristic time course. There is typically a latent period of a few hours (commonly 4–6h) after the UV insult, during which the patient feels normal[22][5]. After this delay, symptoms rapidly escalate. Early signs may include mild irritation, scratchiness or burning; soon this progresses to severe pain, tearing, redness and light aversion. Patients often awaken from sleep with intense eye pain following a bright day without protection.

Peak symptoms occur within the first 12–24 hours after exposure. The pain is often described as sharp, stinging or burning, and it typically worsens with blinking[14][5]. Bright light (even indoor lighting) becomes unbearably painful (photophobia). Other common complaints are blurred or hazy vision, tearing, eyelid swelling, and headache or nausea from the discomfort[31][15]. Patients frequently report a feeling of an abrasive foreign body in each eye. Anxiety and restlessness are natural responses to the intense, constant pain.
Fortunately, photokeratitis is self-limited. Within 24–72 hours the corneal epithelium regenerates, and symptoms resolve as the surface heals[6][19]. Typically, vision returns to baseline without sequelae. Uncomplicated cases leave no lasting damage. Only in very severe cases (prolonged exposure without treatment) might transient stromal edema or superficial scarring occur, but this is rare. Recurrent photokeratitis (frequent “snowblindness” episodes) can accelerate chronic ocular surface diseases (pterygium, conjunctival changes) and contribute to cataract formation over a lifetime[12][13].
Typical timeline: Initial symptoms can start as early as 30–60 minutes or as late as 12 hours post-exposure[32][22], usually peaking around 6–12 hours. Symptoms gradually improve by the second day and are often gone by 48 hours[31][19]. The corneal epithelium generally re-forms within 1–3 days[6]. If untreated or if UV exposure continues, the course can be more protracted.
Symptoms: Patient Experience
Patients uniformly describe severe bilateral eye pain. Common descriptors include “like sand or glass in the eyes,” burning, stinging or intense pressure[4][3]. The pain is often worse when opening the eyes or blinking. Even ambient indoor light may be intolerable – patients typically keep their eyelids squeezed shut or wear dark glasses. Tearing is profuse and constant, as the eye tries to “wash out” the perceived irritant[33][22]. Many note blurry or washed-out vision, sometimes seeing halos or colored fringes around lights (from corneal edema)[31][34]. A dull headache or brow pain is common due to reflex squinting and stress[15][31].
A patient-oriented summary of typical sensations:
- Sharp, burning eye pain in both eyes, often described as the worst ever. Pain is usually equal in both eyes and worsens with light or touch[14][22].
- Photophobia: even dim light causes spasm of the eyelids and aggravates pain. Patients may note that turning off all lights is the only relief.
- Tearing and redness: eyes water continuously (reflex tearing) and look very bloodshot. There is often mild eyelid swelling due to irritation.
- Foreign-body sensation: a constant feeling that sand, soap or grit is under the eyelids, even though none is present[4][22].
- Vision changes: usually mild blurring or fogging, transiently reducing acuity. Some describe seeing halos around lights or a slight color wash.
- Headache/anxiety: intense ocular pain can cause headaches, nausea or panic until the patient understands the cause.
These symptom descriptions are consistent across case reports and patient narratives[14][22]. Importantly, the pain is out of proportion to any observable injury on cursory exam – it is the exposed corneal nerves driving the agony.
Objective Signs and Diagnosis
Clinical diagnosis relies on history and exam. Key clues are a history of recent intense UV exposure (e.g. skiing, welding) and the delayed onset of classic symptoms[5][22]. On examination: the eyes are typically bilaterally involved. Conjunctival injection (diffuse redness) is present[35][36]. Eyelid skin may be sunburned or erythematous if exposed. Pupils are often small (from bright light), but fundi are normal. Visual acuity is usually full or only slightly reduced.
Slit-lamp examination with fluorescein dye is diagnostic. It reveals numerous pinpoint epithelial defects across the cornea (especially the interpalpebral zone)[16][36]. These punctate erosions may coalesce in severe cases. Fluorescein staining appears as scattered green dots under cobalt-blue light[16]. The cornea may show mild edema and a “ground glass” appearance, but no infiltrates. The anterior chamber is quiet (no cells). These findings contrast with conjunctivitis or dry eye: for instance, photokeratitis spares the palpebral conjunctiva and has a rapid, symmetric onset[37]. (In viral conjunctivitis the redness is more focal, starts in one eye, and has more discharge.)
In summary, diagnosis rests on combining the scenario and exam[5][22]. For example, one case report notes: “patients presented with pain, tearing, foreign body sensation, photophobia and blurred vision in both eyes 4–12 hours after UV exposure”[38]. When those symptoms are seen with punctate corneal staining, photokeratitis is confirmed.
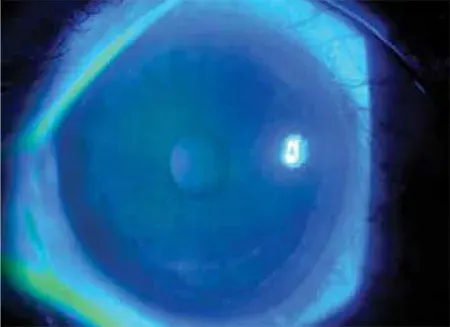 Figure: Slit-lamp photograph under cobalt-blue light after fluorescein instillation (from a photokeratitis case). The scattered green spots are areas of corneal epithelial loss. In photokeratitis, the damaged epithelium takes up fluorescein dye, highlighting punctate erosions[16].
Figure: Slit-lamp photograph under cobalt-blue light after fluorescein instillation (from a photokeratitis case). The scattered green spots are areas of corneal epithelial loss. In photokeratitis, the damaged epithelium takes up fluorescein dye, highlighting punctate erosions[16].
Treatment and Prognosis
Photokeratitis treatment is supportive, as the injury heals on its own. First, remove all UV sources (go indoors, turn off tanning or UV lamps) and stay in a dim environment. Doctors recommend lubricating eye drops or ointment around the clock to keep the cornea moist. Cool compresses or wet dressings over closed eyes can soothe pain. Over-the-counter oral pain relievers (NSAIDs like ibuprofen or acetaminophen) help with discomfort. Special topical anesthetic drops should never be used long-term, as they can delay epithelial healing or even precipitate corneal melt[18].
A prophylactic antibiotic ointment (e.g. erythromycin) is often applied to protect the exposed corneal surface from infection[39]. No eye patching or bandage contact lens is needed – in fact, standard teaching is not to patch, as oxygen promotes healing[40]. Cycloplegic drops (dilating drops) are not generally indicated, since intraocular pain is minimal and vision is not controlled by focusing. Contact lens wearers should remove lenses immediately and avoid re-wear until fully healed.
With these measures, recovery is rapid. Most patients report dramatic improvement by the second day. The epithelium typically re-forms in 24–72 hours[6][19]. By 48 hours, symptoms usually have almost completely resolved[31]. Follow-up with an ophthalmologist is optional if recovery proceeds normally; any worsening or persistence beyond 72 hours should prompt re-evaluation.
Prognosis: The outcome of a single photokeratitis episode is almost always excellent. Vision returns to baseline, and there is generally no scarring because only the superficial cells were lost. (Rarely, small subepithelial haze or slight astigmatism can persist if the central cornea was severely eroded.) One case series notes that by 2 days post-injury all examined corneas were fully clear[41]. Long-term vision loss does not occur from an isolated UV keratitis. However, the episode is a warning: each such UV insult adds to lifetime eye damage. Chronic or repeated exposure to UV – especially without protection – contributes to pterygium formation, cataracts, and malignancies of the conjunctiva/eyelids[12][13]. Thus, the emphasis after recovery is prevention.
Prevention and Protective Eyewear
Snow blindness is entirely preventable with proper UV protection. The cornerstone is high-quality sunglassess or goggles that block 99–100% of UVA and UVB (often labeled “UV400”). Wrap-around frames or goggles with side shields are preferred, as they block sunlight and reflected rays coming from above or the periphery[21][20]. The American National Standards Institute (ANSI Z80.3) sets minimum UV-blocking requirements for sunglasses – look for ANSI or CE certification and “UV400/100% UV” markings[20][30].

Lens darkness (visible light transmission) is a separate issue. For bright sun and snow glare, darker lenses (VLT ~10-20%) are recommended so that pupils stay constricted; for skiing in shade or low light, a lighter tint with 50%+ VLT is acceptable. (Importantly, lens color and darkness do not guarantee UV protection. Only the UV-rated specification matters[42].) Polarized lenses are especially useful for water glare but can sometimes reduce contrast in snow (possibly hiding icy patches) – many winter eyewear combine UV-blocking polarized lenses.
Additional measures: wearing a broad-brimmed hat or cap blocks ~50% of ambient UV reaching the eyes. UV-blocking contact lenses (Class 1 or 2 UV absorbers) can supplement protection by preventing peripheral UV entry, but they cannot substitute for sunglasses (they do not protect the eyelids and conjunctiva[43]). Finally, be mindful of cumulative exposure: even on cloudy or low-sun days, snow/sand reflection can induce burns. It’s wise to use sun protection consistently during ski/snowboard trips or beach time[20][44].
Eyewear specifications: Look for “100% UVA/UVB” or “UV400” rating[42]. Wraparound styles or snug goggles block off-axis light[21]. Coverage that extends close to the brow and cheekbones is ideal. Check that the lens material is shatterproof (polycarbonate) if engaging in sports. Always reapply protective eyewear on demand (don’t lift goggles when going through sunlit sections). In workplaces with UV hazards (welding, germicidal lamps), use certified face shields or goggles with the appropriate shade and impact rating.
With these precautions, snow blindness can be prevented. In polar or alpine regions, classic Inuit-style carved goggles (narrow slits) were an early but effective solution[30]. Today’s recommended eyewear carries the same principle: block as much stray UV as possible.
Surface UV Reflectance Comparison
| Surface | UV Reflectance (% of incident UV) |
|---|---|
| Fresh snow | ~85 (range ~60–94%)[8] |
| Ice/snow pack | 7–75 (depending on age/clarity)[8] |
| Sand (light desert/beach) | ~25 (up to 25%)[8] |
| Water (calm sea) | ~5 (0.6–5%)[9] |
Comparison of typical UV reflectance of common outdoor surfaces. Note that actual values vary with sun angle and surface conditions. Fresh, clean snow has by far the highest reflectance, magnifying UV dose to the eyes[8].
Sources
[1] [3] [6] [10] [12] [16] [30] [32] [35] [37] [39] [40] Photokeratitis - EyeWiki
[2] [7] [8] [18] [21] [26] [27] [28] [31] [43] [44] Photokeratitis induced by ultraviolet radiation in travelers: A major health problem - PMC
[4] [14] [15] [33] [34] UV Eye Burn (Photokeratitis) – Specialty Vision
[5] [25] [38] [41] Four Cases of Pediatric Photokeratitis Present to the Emergency Department After Watching the Same Theater Show - PMC
[9] Ultraviolet Radiation Albedo and Reflectance in Review: The Influence to Ultraviolet Exposure in Occupational Settings - PMC
[11] [13] [19] [20] Photokeratitis: Symptoms, Causes and Treatment Options
[17] [22] [23] [24] [36] EyeRounds.org: Ultraviolet Keratitis
[29] Is Your Medication Making Your Eyes Sensitive to the Sun?
[42] Reflected UV: Eye Safety for Water & Snow Sports - Lensmart